|
Gefangenschaftskrankheiten beim Elefanten Captivity
Disorders in Elephants D.A. Fagan,
J.E.Oosterhuis, and A. Roocroft. |
|||||||||||||||
|
FUNDAMENTAL TUSK STRUCTURE The elephant's tusk is another of those ingeniously designed mammalian body parts, which functions quite adequately in the environment for which it was designed, but Gefangenschaftskrankheiten symptoms can appear with joyless regularity in the lives of captive animals. Of course, this circumstance is not unique to elephants. It is well known that walruses do not fare any better, when their tusks are used to retrieve mollusks at the bottom of a concrete swimming pool. Nor do the Babirusa's tusks survive long when used to persuade concrete or steel to move aside. But, since there are now, and will no doubt continue to be for some time to come, tusked elephants in captive environments, it is important to understand this most unique, protrusive, anterior denticle, and its unusual nature, which has been discussed by numerous authors including Colyer, Miller, Perry, Stannus, and Weatherford. Zoologists have documented the effect of tusk weight and growth on the entire upper torso of the elephant. Noteworthy is Kingdon's description of the relationship of tusk to musculature and skeletal structure. "The elephant has tall thoracic spines sloping back to take the strain of the heavy head, their length and form are correlated with the weight of ivory carried, and the back of the skull has an enlarged area for the attachment of big neck muscles. In the old elephant the arrangement may be likened to balancing scales with the forelegs acting as a fulcrum, whereas in the younger or tuskless animal a bridge is more apparent, as the head is relatively light and most weight is spread behind the front legs." (Kingdon, 1974, p.84) Building on this notion of musculature, Kingdon further elaborates on differentiation of tusked and tuskless animals, "A comparison of the skulls of elephants with and without tusks reveals that the heavy-tusked skull need strong buttressing to hold the base of the tusks, and also it reveals that the weigh imposes stresses, and muscles are developed so that the whole form is altered in almost every particular." (Kingdon, 1974, p.93) These thoughts situate the status of the tusk within the overall context of the elephant's physiological development. However, specific attention to the tusk itself is clearly indicated. The elephant's tusk is, as Sognnaes suggests, just another large example of an extremely well vascularized continuously growing tooth containing a readily identifiable ivory core. It has two centers of growth. The first is axial growth, which originates solely around the apex of the tooth, and which results in all of the eruptive force of the tusk, much like the 'nail bed' is the sole source of eruptive growth of a toe or finger nail. The second center of growth is radial or radicular growth, and represents the thickening of the internal axial wall of dentin directed toward the internal center line, or long axis, of the developing tusk (see Fig. 15). All mammalian denticles, including tusks, are "outside" structures like hairs and/or toe-nails. However teeth are "embedded" into an indentation or invagination into the bony alveolar process of the jaws, and cantilevered out of the animal's body in order to function. Anatomically, the teeth of mammals are held onto the animal's body by a ligamentous form of joint known as a gomphosis. Teeth are actually held in place in the same fashion as all of the animal's other joints. They are attached to the bone of the animal's jaws by a ligament known as the periodontal ligament (PDL), and have more in common with the elephant's knee joint than with its toe nail.
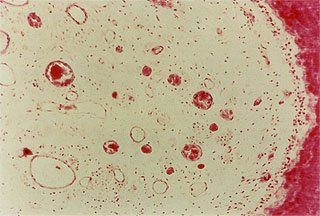
All mammalian teeth have two blood supplies, as do tusks. The first - or blood supply to the tusk's dental pulp enters through the large, open apex below the elephant's eye in a complex, multi-vascular pattern. The gelatinous textured soft tissue within the tusk is properly referred to as dental pulp tissue, and in the elephant the dental pulp is extremely well vascularized all the way to the internal tip of the tusk, where it is known as the pulp horn (see Fig. 16). The second vascular source to the tusk reaches the tooth through the periodontal ligament originating from the surrounding bone. This blood supply does not actually enter into the tooth, although intracellular fluids can flow osmotically through a healthy periodontal ligament into the dentin tubules system within the dentinal wall of the tusk and into the pulp chamber under certain circumstances. This dual blood supply is the basis for the success of traditional endodontic or root canal therapy. This accounts for the fact that the blood supply of the tooth can be obstructed, restricted, or eliminated by endodontic procedures, and yet the tooth will remain in the mouth and continue to function relatively normally.
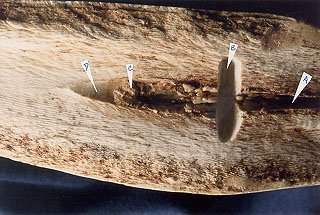
When the elephant's tusk is rapidly abraded, fractured, sawed off, or is traumatically split in any manner such that the pulp is exposed, the "inside / outside" barrier of the animal's body is breached, and immediately microbes invade and infect the pulp tissue. A broken tusk with an exposed pulp chamber is an open wound, and should be treated as such. Even if the pulp is not exposed directly to the outside of the body, it can become overheated by any mechanical cutting device or process, and suffer an internal burn-like injury. In work camps in India, tusks are traditionally cut underwater in order to avoid this sort of internal "burn" injury (see Fig 17). The tusk reacts to any injury with almost exactly the same inflammatory response that occurs elsewhere in the animal's body; that is with increased blood flow, blood pressure, temperature, and loss of function.
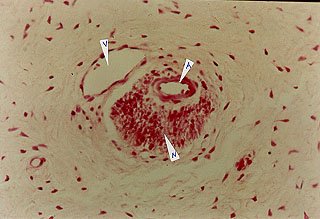
In instances where the tusk fractures below the gingival crest, there can be a great deal of pain and discomfort associated with the sharp edge of the underlying tusk as it continues along its pre-determined erupting path through the surrounding, overgrown, or hyper-plastic gingival tissue. Although in humans and many other mammals, a fractured tooth is an immediate source of great pain, an elephant does not seem to notice or react to an exposed pulpal injury to its tusk. Elephants behave as if there were no pain associated with pulp tissue injury. The authors recently documented the explanation for this behavior, by demonstrating that there are "no nerve tissues within the dental pulp of elephant tusks or molars" (see Fig. 18).
Moreover, the tusk's dental pulp tissue is so well vascularized that the animal's natural immune system mediated defensive mechanisms immediately mobilize, attack and often defeat the initial infection, and proceed to isolate the injured pulp tissue by forming a protective secondary dentin bridge. This process is similar to the classic foreign body reaction seen throughout the remainder of the body. This self-repairing mechanism of dental pulp is well documented in all healthy mammalian teeth. Obviously its success depends upon such issues as the virulence of the invading organism, the severity of the exposure, and the health of the tissue. Clearly, it does not always succeed. There are many broken tusks known to us all exhibiting chronic, suppurative, necrotic pulpitis, eventually destined to be lost. Resolution of this potentially chronic dental infection of the tusk has been described by numerous authors including Allen, Driver, Kapustin, Kertesz, and others. The treatment alternatives are all generally time-consuming, expensive and frustrating. It is however, possible on occasion, to resolve the broken tusk problem quickly and naturally by taking advantage of the tooth's natural self-repair capability - the secondary dentin bridge formation mechanism. With the help of a small amount of conventional dental care, the bold clinician can dramatically influence the outcome of this all-too-common tusk injury (see Fig. 19). This often utilized, traditional dental therapy is described in the literature as the vital partial pulpotomy. It has been copiously described in the human dental literature, has a good history of success in many exotic animals with continuously growing teeth, and has been successfully applied to elephant tusk injury by Bush et al., Fagan et al., and many others. Here again, a well-timed ounce of prevention, in the form of the prompt bold application of a proven dental therapy, is worth much more than a pound, if not ten thousand pounds of cure.
|
|||||||||||||||
|
For translation information and instructions, please CLICK HERE. http://www.colyerinstitute.org
This web site is best viewed with a browser setting of 800 x 600 or greater. If you use a smaller screen size and would like to view the content of this site using an alternate interface, please click here.
|