|
Gefangenschaftskrankheiten beim Elefanten Captivity
Disorders in Elephants D.A. Fagan,
J.E.Oosterhuis, and A. Roocroft. |
||||||||||
|
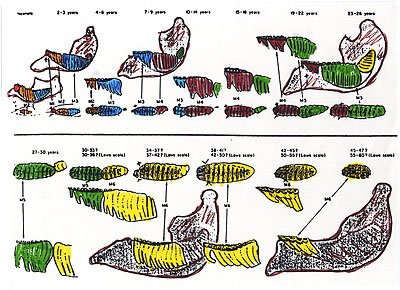
GEFANGENSCHAFTSKRANKHEITEN and MOLAR MAL-POSITION In both African and Asian elephants, molar dentition is considered unique in a variety of ways. These include: species specific original design, dental formula, process of development, eruptive sequence, consequence of wear upon replacement, impact of diet upon development and method of eventual loss of dentition. Unlike all of the other mammals, during their normal life span, elephants form six sets of teeth in each quadrant of their mouth for a total of 24 molars, each erupting in a sequential pattern, as required. ( see Fig. 10)
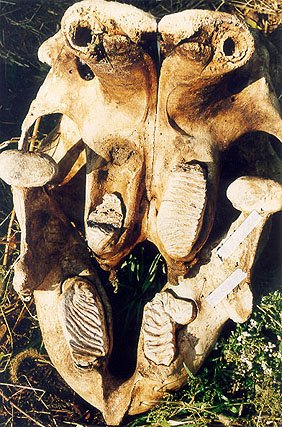
Ideally, this progression of developing molar teeth would provide four functional molars present in the elephant's mouth at any one time; i.e., one per quadrant or arcade. However, since the development, wear, loss and replacement rate within each elephant's mouth is such an environmentally sensitive and dynamic process, dependant upon so many unpredictable factors, this is usually not what happens. Normally, any individual elephant may have as many as three whole or partial molars visible and functional in any one quadrant of its mouth. In addition, the rate of eruption, wear and loss of the elephant's molar teeth rarely occurs in the same identical time frame on both sides of its mouth. Most oral cavities are not bilaterally symmetrical. This is because elephants, like humans, generally exhibit a preference for one side of their bodies or the other, and have a "dominant side", which sustains most of the wear and tear. This often includes a preference for chewing more often on one side of its mouth. As the molar teeth are methodically abraded away and finally lost, their replacement molars have already taking shape, are developing, and mineralizing directly behind the "in-use" molar. Properly referred to as a succedaneus tooth, this next developing molar is slowly moving forward within the body of the alveolar process into position to substitute for, or replace its predecessor, when needed. Within different geographic environments, the rate of growth and replacement of these molars has obviously evolved at a different rate over time, as has the entire elephant. The customary rate of tooth attrition found within a specific habitat is determined by the natural abrasivity of the food found within that specific habitat. Change the abrasivity of the elephant's feed too much, and the animal is sure to develop dental malocclusions, because its pre-programmed rate of dental growth and molar eruption schedule is no longer in synchrony with its dental attrition rate. Although general anesthesia is often required to adequately examine an elephant's molar malocclusion disorder, it tends to originate unilaterally in the mandible, when one of the "in-use" molars does not abrade away at the anticipated rate. However with the passage of time, the most commonly visualized first clinical sign of malocclusion is the mal-positioning of the opposing maxillary molar. Even though a molar may fail to exfoliate as planned, its developing successor or replacement tooth continues to develop, grow and mineralize at this animal's genetically pre-determined "normal" rate. Normal abrasive wear and tear erode away the molar(s) "in-use", while the eruptive forces produced by the growth of its succedaneus tooth continues to push the "in-use" molar forward until it is exfoliated or finally comes into contact with the cortical plate of bone shaping the anterior wall of the mandible. When the "in-use" tooth is no longer able to drift or erode away, the cortical bony contour of the alveolar process then begins to direct the "in-use" tooth aside until it finally becomes impacted or wedged into a position from which it can no longer move (see Fig. 11). At this point, the forces necessary to cause necrosis of the bony cortex exceed the eruptive forces of the developing tooth, and complete impaction has occurred . Even the soft, partially-mineralized, un-erupted, developing molars can become "disfigured and/or deformed" by this process (see Fig. 12 ). An impacted molar is usually inclined medially because of the strong influence of the animal's lip and cheek musculature, and often is accompanied by supra-eruption of the tooth. This process is much like the drifting of logs or icebergs down-river with the flow of the current until they become obstructed into a logjam or icepack. This impacted or mal-positioned molar now tends to become periodontally infected following the impaction of food matter, and in time will become periodontally and/or peri-apically abscessed requiring extraction therapy (see Fig. 13 ).
The first clinical sign of a functionally significant molar malocclusion, aside from the visually obvious mal-positioning of the teeth, which may or may not be apparent through causal observation, is a change in the texture and coarseness of the animal's fecal mass usually associated with weight loss. These subtle changes will almost always occur gradually over a period of time, and unless one is experienced at carefully observing each individual and the fecal appearance of well masticated feed, modest early changes are easy to overlook (see Fig. 14). A change in fecal consistency is a direct and absolute indication of a change in the masticatory efficiency of the animal. These changes are always an early indicator that more diagnostic analysis is required, and the most common sign that the oral cavity contains a mal-positioned molar, which should be corrected or removed.
The removal of an elephant's molar tooth is always a difficult surgical undertaking, although it has been performed successfully on numerous occasions, and described by a number of author's including Allen, Bush, Driver, and Kertesz. All successful molar removal techniques adhere to the proven principles of oral & maxillofacial surgical extraction theory with a proportional adjustment to accommodate the extraordinary size of the elephant's tooth. The soft tissue is detached and protected, a "moat" is created around the tooth into the alveolar process, elevating and loosening forces are applied as indicated. The tooth is then removed. The socket site cleaned, and treated as an open wound until completely healed. The healing process can be assisted by flushing the surgical site several times a day with a directed stream of water, medicated if possible. The earliest published report of an elephant molar extraction procedure occurs in the British literature in 1884. Sterndale also provides a description of molar dental treatment by sawing off a portion of the offending tooth in a fully conscious, physically restrained adult elephant in "Seonee" in 1887. Although a number of authors including Humphreys have commented upon the issue of "constant pain" from a tusk related "toothaches", it has been shown by Fagan et al, that sawing off the tusk can not per se hurt the animal, as there are no pain nerves in the elephant's dental pulp. An untreated infection within the tusk can however cause great pain once it reaches the apex of the tusk and spreads into the surrounding alveolar bone.
|
||||||||||
|
For translation information and instructions, please CLICK HERE. http://www.colyerinstitute.org
This web site is best viewed with a browser setting of 800 x 600 or greater. If you use a smaller screen size and would like to view the content of this site using an alternate interface, please click here.
|